
19 . 04 . 2019
Case Report - Fatigue and "Hypoglycemia"
The following is the case of a 45-year-old female patient, C.M., whose chief complaints were chronic disabling fatigue and episodes of exacerbated weakness that had been interpreted as probable hypoglycemia. The situation was reversed with diet changes and supplementation.
C.M.’s symptoms had been worsening for a year, coinciding with a particularly stressful phase at work with frequent traveling. She had already experienced a similar situation in 2003. At that time, C.M. was evaluated in an inpatient setting for hypoglycemia and workup of an eventual insulinoma (an insulin-producing tumor that can cause sudden drops in blood glucose). This hospitalization was inconclusive.
On the initial appointment, the chief reported symptoms were:
- fatigue and weakness, mainly 2-3 hours after eating;
- dizziness;
- irritability;
- insomnia;
- afternoon headaches;
- low resistance to stress.
This presentation was typical of glycemic dysregulation and suggested an imbalance in the functioning of the hypothalamic-pituitary-adrenal axis. The adrenal glands are responsible for producing cortisol in response to stimuli from the hypothalamic-pituitary axis, which is located at the base of the brain and functions as the great conductor of hormonal balance in the body.
During the first visit, the patient’s diet was analyzed and was found to be very rich in refined carbohydrates (bread, biscuits, crackers, etc.). C.M. used these foods as a fast source of energy to try to alleviate the fatigue. However, these acellular carbohydrates (from sugars and flours) have a counterproductive effect because they generate a very erratic glycemic curve with many ups and downs, particularly when they are not ingested with fat or protein. A grain-free diet, with fruit and tubers as the primary sources of carbohydrates, was recommended. The consumption of protein at breakfast due to its stabilizing effect on blood glucose was also advised.
After two months, C.M. reported an 80% improvement in symptoms due only to diet adjustment, which she implemented with discipline.
Blood tests revealed an iron deficiency, with no evidence of anemia, and insufficient vitamin D values.

Fig. 1 – Relevant findings in the laboratory evaluation after the initial consultation.
Hormonal testing revealed insufficient cortisol levels. Cortisol is a vital hormone with several functions, such as inflammation suppression, blood pressure maintenance, and hypoglycemia prevention. In extreme situations, the adrenals do not produce any cortisol despite being stimulated by the pituitary, a condition known as Addison’s disease, whose main symptoms are profound fatigue, hypotension, and weight loss. The latter was not C.M.’s case, in whom cortisol levels were not that low.
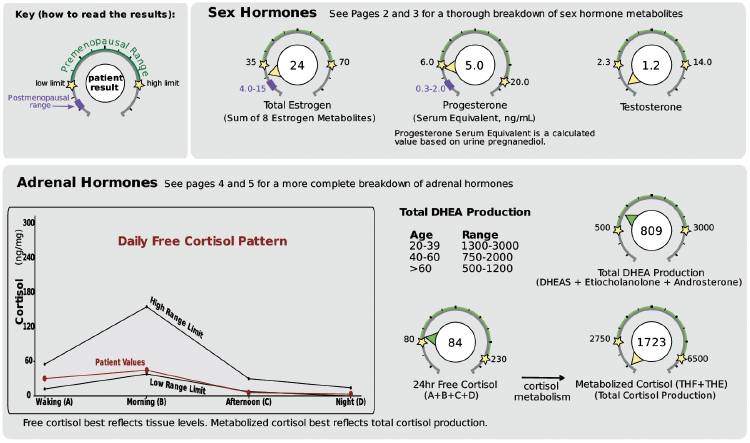
Fig. 2 – Urine hormonal testing with free and metabolized cortisol measurement.
At this stage, supplementation with glandular extracts and adaptogens was recommended. These compounds have a modulating effect on the production of cortisol. Iron and vitamin D deficiencies were also corrected. Symptoms continued to improve, but at a later stage, it was decided to support the production of androgens (male sex hormones which also exist in women), with a low dose of DHEA (dehydroepiandrosterone), to correct the testosterone deficiency.
Despite not having acted directly on the female sex hormones, their values also normalized once the hypothalamic-pituitary-adrenal axis was rebalanced, which attests the interdependence of these hormonal systems.
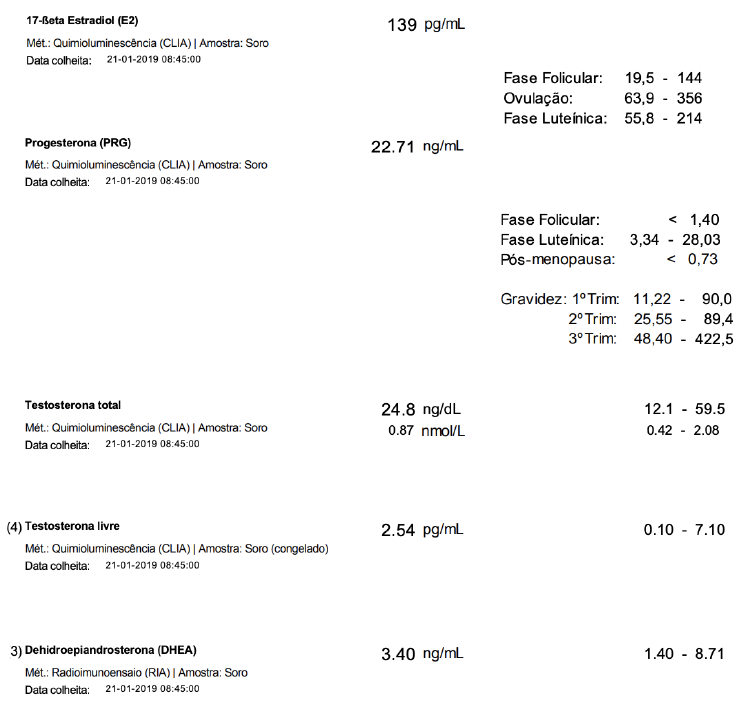
Fig. 3 – Laboratory evaluation after the 3rd consultation.
This was a case of hormonal dysregulation induced, mostly, by a diet rich in acellular carbohydrates that leads to blood sugar imbalances. The professional stress to which C.M was subjected probably also contributed to the worsening symptoms since it overwhelmed an already fragile system. Through an integrated plan, which included directed supplementation, it was possible to control this process and increase this patient’s quality of life.